

One pandemic is, obviously, COVID19. The other is the massive, global burden of chronic diseases that have been siphoning years from lives and life from years for the past half century and more- and will be doing so long after COVID19 is archived in history books.
Why are two concomitant pandemics good news, rather than bad? Well, if the toll of SARS-CoV-2 pertained to the virus and nothing else, there would be little we could do about it other than shelter from exposure by various means; scramble for a vaccine with unprecedented alacrity; and hope for the best. If COVID19 were an equal opportunity menace, we would all be comparably at risk, and that risk would derive from the virus itself. The “fault,” as it were, would lie with SARS (only), not with ourselves, our culture, and such benighted misadventures as the routine acceptance of “junk” as a food group.
The bottom line is that if a viral contagion were preying upon people with a baseline health that could not be improved- then the pandemic toll would be the toll, for thee, and me, and everyone else – and our one and only choice would be to pay it.
If, however, the contagion preys preferentially on the frail- like those predators we’ve all come to know watching nature shows- and some of that frailty is remediable- then there is an opportunity in the crisis of COVID19.
And so it is. The relevant frailty is in large measure age-related, and that- we cannot fix. We cannot undo old age. But on the other hand, we can also accept that every kind of mortality risk is concentrated among the elderly for the simple reason that we are all mortal. Eventually, we will all die- and most of us will do it old, and because we are old.
That in no way obviates the grieving and mourning for the pandemic losses of elderly loved ones so many of us have experienced. My condolences extend to all of us so affected. Elderly people are, though, more prone to die, pandemic or no, and nothing less fundamental than our mortality requires us all to come to terms with that.
The relevant frailty is also, in its other large measure, modifiable; it is a consequence of prior chronic disease. Cardiovascular diseases, type 2 diabetes, hypertension, and obesity are all effectively “pandemic,” or at best hyperendemic throughout the modernized and modernizing countries of the world. These in turn are ill effects of adverse lifestyle practices– especially, although not only, poor diet quality and lack of routine physical activity. We have known the salience of these, and the other root causes chronic morbidity and premature mortality for more than a quarter century at least; we have known how to eliminate 80% or more of this burden for as long.
Why haven’t we? There are many reasons, of course, but among them is this: chronic disease is chronic, at least until it becomes acute (e.g., as when heart disease advancing slowly for years or decades suddenly precipitates a massive heart attack, or sudden cardiac death). The chronic is a slow-motion menace that quite simply does not capture our attention, concentrate our anxiety, stoke our desperation for remedies, or activate our fight-or-flight response. COVID, however, in its acute assault on our communities, in its onslaught of breaking news…does all of that.
The two- chronic diseases, the acute threat of COVID- are mechanistically conjoined especially through the diverse ramifications of inflammation. Obesity, diabetes, and cardiovascular diseases both induce systematic inflammation, and are propagated by it. Such dysfunctional inflammation in turn impairs the body’s capacity for the functional inflammatory responses that are the hallmark of effective immunity, while potentiating misdirected, unbalanced immune responses such as the now notorious “cytokine storm.” These pathways impair vascular function at the origins of its control in the endothelium that lines our vast network of blood vessels, putting every organ-system at risk, and explaining the dizzying spectrum of COVID complications.
In this calamitous interplay of pandemics new and long established- lies the opportunity. Much of what places us at higher risk for bad COVID outcomes is fixable, and COVID gives us a shared, potent motivation to fix it. This, in other words, is what we in Preventive Medicine call a “teachable moment.” The healthy, balanced immunologic responses of generally healthy bodies are an obviously high-potency defense against the ravages of SARS-CoV-2. Why race for the extrinsic salvation of a vaccine while neglecting the rarefied, intrinsic defenses of our native immune system, granted the conditions that allow it to thrive?
The policy implications of this are much as they have seemed from the start; our risk for severe COVID infection varies widely, and our interdiction efforts should correspond to avoid hurting those we aim to protect, and protecting those who most need it far less than we should. The personal implications are simply this: there has never been a better time to get healthy.
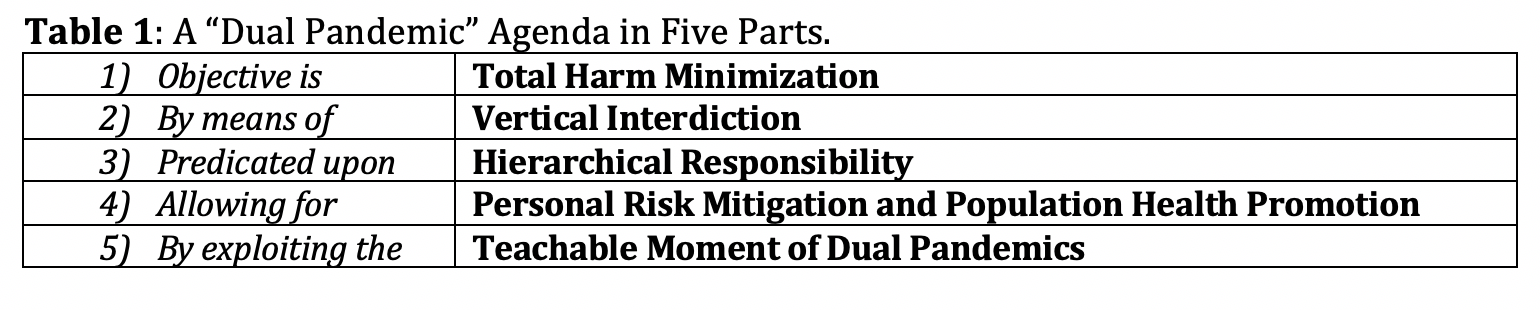
My vision for this agenda, shared between the domains of public accountability and personal responsibility, spans five components. (1) The policy objective is total harm minimization (THM), reducing to the irreducible minimum the cost in health, lives, and human potential of infection and misdirected interdiction efforts alike. (2) The primary tactic in the service of THM is “vertical” or risk-based interdiction, the direction of interdiction services, policies, and practices differentially and in accord with population-specific risk tiers (see Figure 1, below). (3) The above tactics should issue from an over-arching strategy of hierarchical responsibility, in which governmental authorities establish the general policy framework or architecture for permissible practices; businesses, universities, school districts, churches, and other diverse entities are required to comply with governmental policy directives but are granted maximal latitude in customizing the methods of compliance (an approach already reflected in the “Chinese menu” of CDC recommendations); and individuals are invited to know and manage their personal risk (see Figure 2, below) – including the potential to migrate from one risk tier to a lower one, and thus accrue a new suite of pandemic “liberties.” This would allow for (4) personal risk mitigation, and population health promotion– potentially improving the national vitality in ways that reverberate through everything from personal fulfillment to national security, health care costs to happiness to GDP. The above framework would invite us to (5) exploit the teachable moment of dual pandemics – and come through stronger. This 5-part “dual pandemic agenda” is summarized in Table 1, below.
Figure 1: A COVID19 risk stratification matrix.
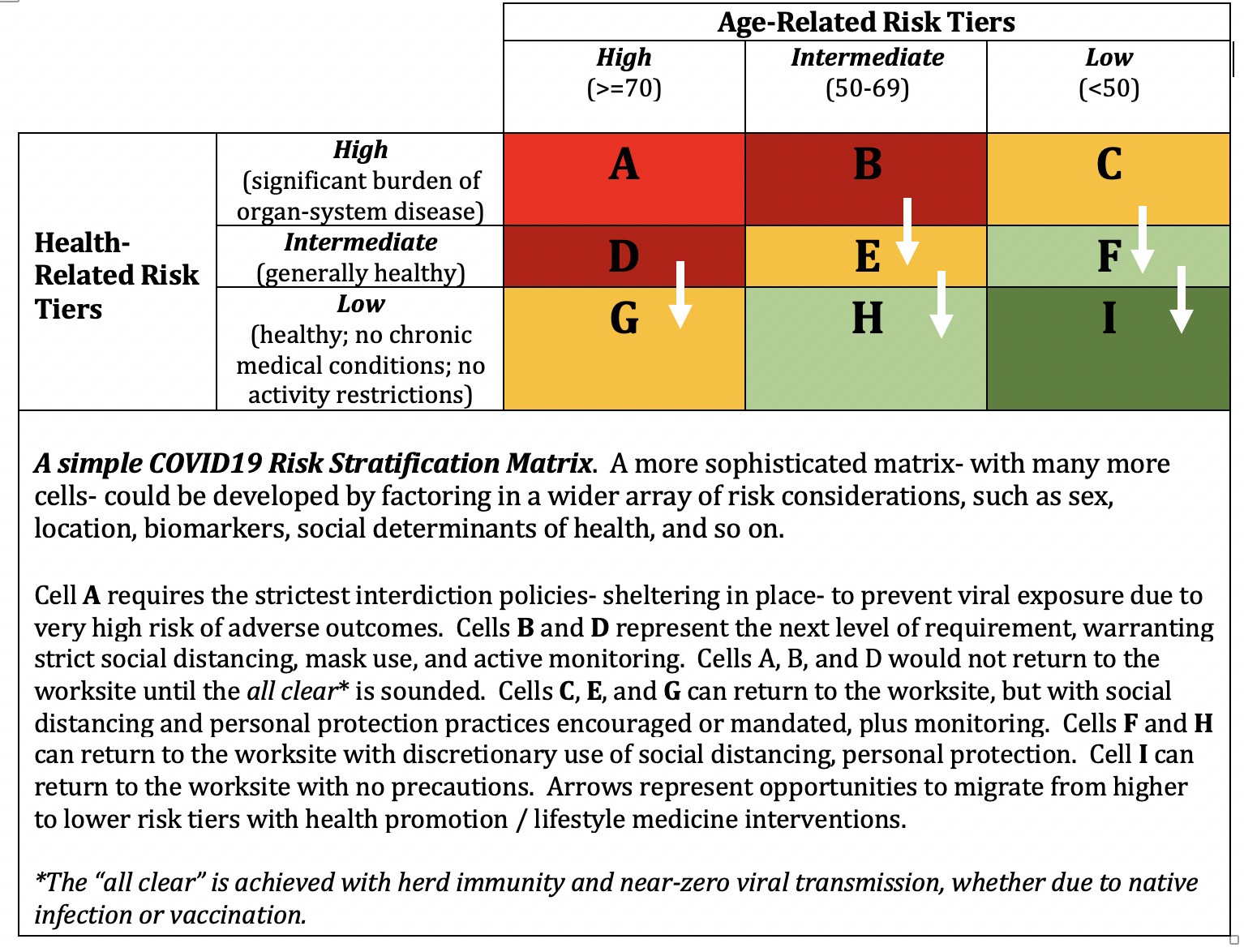
Figure 2: Screen shot of a COVID19 personal risk calculator, courtesy of Everist Health.

One could argue for a still grander confluence of crises, noting- as my friend Tom Friedman has recently done– that our interactions with nature are as out-of-balance and dysfunctionally inflamed as our own beleaguered immune systems; that this imbalance lies at the origin of this pandemic, as it will the next. There is cause to perceive the implications of this pandemic beyond the bounds of our skin, promise in doing so.
But in the service of avoiding bites too big to chew- let’s defer that argument for another time. For now, the horizons within our skin suffice to remind us all that a crisis is a dangerous opportunity. By imposing an acuity of danger that has fixed our anxious attention, COVID19 provides an opportunity to confront the clear, omnipresent, long-established, and much-neglected ravages of chronic disease.
Two pandemics are, paradoxically, better than one- when each evinces an opportunity to slash the human costs of the other.
-fin
This article was first published on LinkedIn.