

I had hoped the pandemic might be winding down now in the United States, and other hard-hit countries. I also noted that when the pandemic does end, it would be very hard to tell for quite some time. Accordingly, a proximal end could yet be materializing, and let’s hope for that- but the rising case counts in much of the U.S. and world argue against it.
The best, current interpretation is that the pandemic is not yet over, even where it hit hardest some months ago, but thus far at least- it is different.
Thus far, there is a vastly greater divide now than at the start of all this between the case count trends, and the casualty trends. Case counts are elevated, but hospitals are not overwhelmed. Cases are spiking, but – thus far, and for the most part with isolated exceptions- fatality counts are not.
Thus, the Mulligan.
Famously, those who don’t learn from the follies of history are destined to repeat them. The follies of our responses to COVID were fatal on an epic scale, so repeating them would be a grave mistake. A resurgence in viral transmission brings with it the chance to get our policy responses right.
As fate would have it, that opportunity coincides with the release of the Great Barrington Declaration, a policy document issued by a triumvirate of epidemiologists from Harvard, Stanford, and Oxford- and as I write this, signed by nearly 6,000 public health professionals (I among them) and over 12,000 medical practitioners from around the world. The document espouses “Focused Protection” of the vulnerable to minimize the harms of lockdown and infection alike. In other words- my words at the start of this– it espouses “total harm minimization” by means of “vertical” or “risk-stratified” interdiction policies. I am happy to go with “focused protection.”
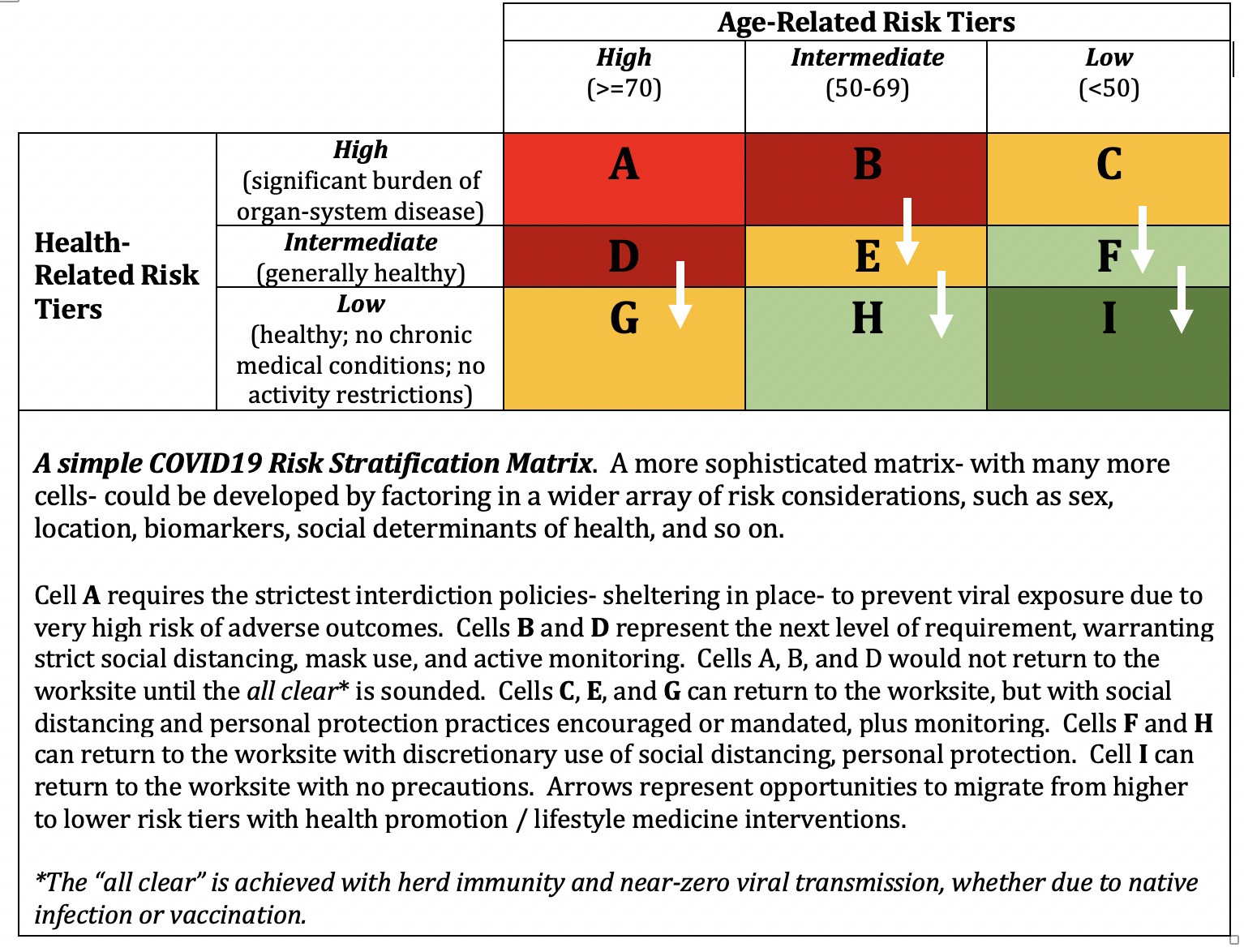
The idea is as robust as it is simple: match the level of protection mediated by practices and policies to the level of risk. Do not over-protect those for whom SARS-CoV-2 is a trivial threat; do not under-protect those for whom it is a lethal menace.
Many countries badly need a pandemic Mulligan to reset misguided policies, but none more than the U.S. which deserves special recognition for our master class in pandemic mismanagement. We- along with only a very few other countries -managed to get everything wrong in both directions.
We locked down too late, too inconsistently, and too inefficiently; opened back up too indiscriminately; and practiced sensible personal protection too unreliably to minimize losses to the virus. And, we locked down too wantonly and too incoherently to minimize the devastating transformation of social determinants of health into, as Health Affairs put it, social determinants of death.
Total harm minimization by means of risk-stratified interdiction policies- focused protection- respects both threats, and aims to reduce both to the irreducible minimum.
That word- respect- is integral to any hope we may have of doing better between now and whatever serves as the decisive end to our pandemic life. COVID deserves, as it has all along, respect.
COVID warrants respect, but not panic. COVID has been given its due by almost no one, as populations have divided, abandoning common ground and common cause to claim instead membership in one of two opposing ideologies, one devoted to panic and catastrophizing, the other to contemptuous disdain.
Both are bad- but since the disdain amplifies the toll and feeds the panic, it is the worse of the two. This delusion of contempt is epitomized at the highest levels of current leadership in the United States, where COVID is met, as Nature herself is met, as the science we rely on to probe the unknown and advance our understanding is met- with a toxic blend of ignorance, derision, and bravado.
But the panic, too, has been misguided, constraining policy options within a strait jacket of sanctimony. The idea has caught on during COVID that any death is a moral failing, and any policy allowing for any death, an act of sociopathy. This is an absurd standard applied to none other among the myriad causes of some 8,000 daily deaths that occur routinely in the United States. We do not lock down the highways because of any one fatality there; we do not close the nation’s schools because meningitis can be contracted there. Living involves risk.
COVID warrants neither disdain nor panic. If inclined to panic over anything, let it be climate change, per the precociously sage counsel of Greta Thunberg. She is quite right that climate change may utterly destroy this planet’s web of life, the treasure of biodiversity. She is quite right that climate change could prove to be an extinction level event for our species. Not the most wildly pessimistic assessment of the COVID pandemic places it even remotely in the same apocalyptic ballpark.
Yes, COVID is bad- or this would all be much ado about nothing. But as bad as the virus is- humble, much-taken-for-granted heart disease kills well over three times as many of us, and does it every year. Poor diet quality- something over which we exercise complete control- kills well over twice as many of us every year as COVID has thus far. If every last viral death is cause for moral outrage, where is that same sentiment with regard to the ravages of junk masquerading as food?
Even the legitimate limits to worst-case COVID projections are ever less likely. We are ever better at treating the infection when that is required; we are advancing toward a vaccine albeit along an uncertain timeline; and we know how to shield ourselves from the virus in the first place, however inconsistently we make use of those means.
Why are case counts rising now? I can think of three potential explanations, one of which comes in two variants.
(1) Some proportion of the new infections among the asymptomatic might be reinfection among those who had an earlier asymptomatic infection and only achieved partial immunity. We know that reinfection can occur after months, and appears to be most likely among those who had mild infection the first time around. This could explain, in particular, high levels of asymptomatic infection on college campuses. This might have been true last February and March, too, but we never tested these populations then.
(2) New cases may be occurring because of higher-than-before exposure doses among those with partial resistance due to prior common cold coronavirus exposure. We know that other coronaviruses confer partial immunity to SARS-CoV-2, but this can likely be overcome with intensity of exposure. Perhaps lapses in mask use, distancing, and/or more indoor versus outdoor exposures are contributing to such occurrences.
(3) Finally, perhaps a surprisingly high percentage of us stayed safely away from the virus until now, despite the want of effective public policies, and only now are exposing ourselves for the first time. This is the one that comes in two variants: (a) this is being done without risk-related precautions; (b) this is being done with risk-related precautions. In other words, if those vulnerable to severe infection now know who they are, they may be far more careful about exposure than those who consider themselves at low risk.
Of the above, 1, and 3b would tend to elevate case counts without elevating casualty counts. Entry 2 is likely a modest contributor to the observed trends, and could be addressed effectively with consistent application of masking, distancing, or both. Only 3a represents an acute peril to be avoided. And, of course, higher case counts are partly a by-product of testing levels massively greater now than they were at the start.
Assuming the pandemic is not about to end before we get the chance, how do we best avail ourselves of our Mulligan opportunity and practice “focused protection”? With four policies, and two personal behaviors.
The policies are:
(1) We can and should use the data we have collated throughout the pandemic to risk-stratify the population.
(2) We should match our policies of protection and viral interdiction to risk- with extreme protections where risk is extreme, minimal protections where risk is negligible (it will never be zero).
(3) The above policies should be standardized nationally, clearly and consistently articulated, supported, and enforced.
(4) We should closely monitor trends with the humility required to make on-the-fly adjustments, either by location or at scale as warranted, to ensure that protection is always adequate and never excessive.
The behavioral translation of “focused protection” involves:
(1) Knowing your personal risk tier, and that of your loved ones.
(2) Protecting yourself and your loved ones in accord with the level of risk.
If the pandemic is already nearly over, then the toll- of infection and social determinants alike- is what it is. It cannot be undone.
If, however, we have some miles to go before consigning COVID to the annals of bad history- we have an opportunity to do far better between here and there. The current divide between cases and casualties incubates the residual hope for total harm minimization by means of focused protection.
We exploit that opportunity by looking both ways before crossing the remainder of the pandemic, and acknowledging the potential harms of infection and social upheaval alike, conceding that both are bad, the prevention of either- a public good.
We exploit that opportunity by giving COVID its due. It is due neither disregard nor panic- just respect.
-fin
This article was first published on LinkedIn.
Dr. David L. Katz is a board-certified specialist in Preventive Medicine/Public Health.
Click here to access the one-page summary of #TotalHarmMinimization
Click here to access the total harm minimization resource library
Click here to access a library of Dr. Katz’ “reality check” videos on the pandemic
Click here to access the Great Barrington Declaration