

The fact is, sadly, and simply- we all are having an Omicron Christmastime. Let’s deal with it.
I am the furthest thing from a radical on this as on all topics. I am, by both proclivity and practice, ill-disposed to extremes of opinion, diatribe where data ought to be, ideology where epidemiology ought to be, and the irritating bark of dogma on any topic.
I say this to establish my alibi, because I fear I am about to sound a bit radical. I think nearly every aspect of our response to Omicron is wrong.
Let’s start with testing, where the demand has been so high that lines are long, supplies are limiting, and many struggle to find tests they think they need or are required to get.
Here it comes: I see little value in widespread testing. Testing is a “form;” its utility requires we answer the question: what is the intended function?
There are two intrinsic functions to testing for COVID, be it Omicron or otherwise. The first is to identify someone who should be separated from the rest of us to avoid spread, and the second is to make a specific diagnosis to guide specific treatment. (A third is to inform epidemiology, but for our purposes here, I will leave that thread to dangle.)
That latter function – specific diagnosis and corresponding treatment- makes sense only when symptoms are present- and only when they are severe enough to warrant considerations of medical care. If symptoms don’t progress much beyond those of a cold, what benefit comes from knowing the specific pathogen? Treatment- which is limited to the customary admixture of rest, fluids, tea, soup and such- would not be affected; it would remain the same for COVID, or rhinovirus. Nor would isolation, since we would generally expect someone coughing, sneezing and feeling miserable to keep their distance from the rest of us until feeling better. Such basic proprieties of coryza and hygiene were in place well before any pandemic.
That leaves the other function: the preemption of spread. But as we are seeing with the truly explosive dispersal of the Omicron variant, its spread is literally inevitable. We are watching something close to exponential transmission. By the time someone tests positive, in other words, they will already have passed it on to others, who will have passed it on to many more others before they, too, test positive. The massive demands of widespread testing in such a scenario is a whole lot of cumbersome form, largely devoid of function. In my increasingly jaded view, it is pandemic theater- fussing over the barn door after the horses have all already bolted.
And worse, because testing has real-world liabilities. If a child in school, or even quite a few children in a school “catch cold,” they are likely kept home until feeling better, but there is never a question of closing the school. But if any such child tests positive for COVID, even if the symptoms are just those of a cold- just such questions arise, amidst consternation and competing passions. Pandemic theater is not a victimless crime.
So why are we, officially, so insistent on a policy with such little advantage in it? I can think of two reasons, both derived from Newtonian physics, which while intended for blocks of flotsam moving through space, seem aptly to capture the antics of clans of humans moving through pandemic decisions. The first is the infamous “equal and opposing reaction.” We began this pandemic here in the U.S. with a dismissive administration directing disdain and derision at the virus, at public health, and at science in general.
Invoking Newton, a response not just opposing but equally ardent exaggerates the place of science and public policy, neglecting the critical role of sense, and applying jackhammers where tweezers would better serve. My concerns about attendant collateral damage are primordial.
The second is simply inertia. Having stewed in the need to contain SARS-CoV-2 for two years, and having largely failed to do so- we now react with more of the same in response to a variant utterly uncontainable. Omicron is going to spread, and short of things the global population would not sanction- truly strict isolation for nearly all of us, Hazmat suits for the rest- we are not going to stop it.
But that is not the gloomy news it may seem for several related reasons. First, hundreds of millions upon millions of us have already had COVID, some of us more than once- so we confront Omicron with partial, naturally acquired immunity. What launches a pandemic in the first place is a pathogen for which we have no or nearly no immunity. We are no longer there.
Second, that naturally acquired immunity has been greatly augmented by effective vaccines. Hundreds of millions upon millions of us have been vaccinated, some of us in addition to native infection. Many have been boosted. None of this makes us impervious to Omicron, but all of it alters our relationship with this bug fundamentally. Omicron finds us with immune systems forewarned and forearmed, and does us vastly less harm as a result. There have long been common cold coronaviruses among us, and Omicron may take up its permanent residence there.
Third, the Omicron variant’s many mutations seem to make it far better at spreading while attenuating its virulence. In other words, it tends to make people less sick. That evidence was just elevated from early hope in South Africa to fresh data from Britain. Combine a less virulent agent with a more immune host, and suddenly we are in the realm of a threat vastly less and different than the one that set all of this mayhem in original motion.
But what about hospitals filling up? We must, of course, take that seriously, and direct policy and personal responses to mitigate it. Doing so requires understanding the cluster of causal factors. First, hospitals always fill up as winter weather propagates infectious diseases along with stresses on hearts and lungs. The vast populations with respiratory and cardiovascular ailments are always at risk of exacerbations and hospital admission this time of year. Any infection in such situations might be the proverbial straw on the camel’s overburdened back.
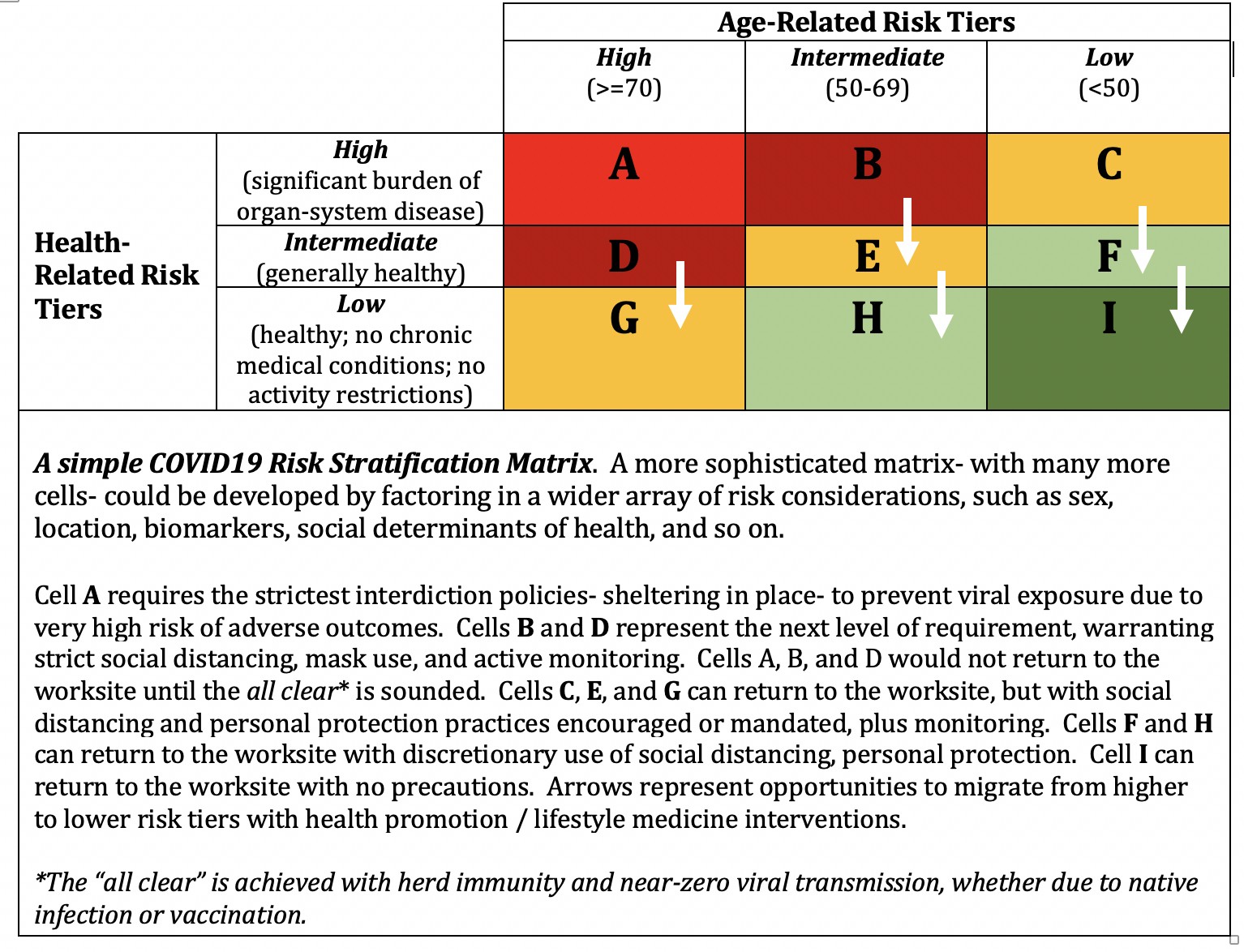
Widespread testing of children in schools with the attendant threat of school closures is not a pertinent response to this problem. Contentious as it has become, for whatever reason, the right response to the risk of hospitalization among the most vulnerable is, indeed, “focused protection,” or risk-stratified pandemic policy. Doctors and patients nationwide, and worldwide, could- and in my view should- be collaborating to determine who is at “high risk” of bad COVID outcomes in the Omicron wave. Such people should get what help they need- visiting nurse services, national guard- to stay home and out of harm’s way until the wave is over. Yes, that’s terrible during the holidays- but it’s better than landing in the ICU. By way of reminder, pandemics are the pits. Once in one, all truly good options have already been foreclosed.
Those high-risk people should be monitored remotely, and daily. At the first hint of symptoms that might be COVID, they certainly should be tested whenever possible. When not possible, for whatever reason, the logical response at present would be to assume COVID. Either way, the newly approved drugs by Pfizer and Merck should be deployed efficiently to prevent the escalation of illness in such cases.
I would very much like to translate this from philosophy to personal practice, and practical advice- but I, obviously, don’t run the zoo. We are all caught up in the inertia and opposing reactions of this fraught, Internet-Age pandemic. If I did run the zoo, I would say: be vaccinated. If vaccinated, and if youth and health place you at low risk, go about your usual business and don’t bother with testing. If you get cold-like symptoms that don’t require any treatment, manage them as you always would, while assuming they might well be Omicron. Keep well away from any frail loved ones for whom you would always do exactly that.
If unvaccinated, get vaccinated- and do your best to keep away from everyone for the next several weeks (the Omicron surge in South Africa crested and began falling in less than four weeks). If frail, elderly, ill- if prone to hospital admission under ordinary circumstances- whether vaccinated or not, stay away from everyone to the extent possible until this is over. You will otherwise be exposed to Omicron. If that does happen, seek testing and treatment at the first hint of symptoms.
As noted, I am not in charge- so my recommendations are hypotheticals. You will, instead, be forced to comply with policies, sensible and otherwise. You will be stuck dealing with form, where function ought to be.
Oh, well. We are, as noted at the start, simply having an Omicron Christmastime; “wonderful” is likely out of reach this year. But we could be safe, and a bit merrier into the bargain, I think, if science and sense would reconcile, and if Santa would take back the reins from Sir Isaac- and push inertia and reactionary opposition off his sleigh.
-fin
This article was first published on LinkedIn.
Dr. David L. Katz is a board-certified specialist in Preventive Medicine/Public Health.
Click here to access the one-page summary of #TotalHarmMinimization
Click here to access the total harm minimization resource library
Click here to access a library of Dr. Katz’ “reality check” videos on the pandemic