

The trip, to Ohio, was arguably ill-timed, given the current trends in viral transmission. Of course, this conference was planned long before the current trends set in, and when it seemed that gradual resumption of life as we knew it before might make sense by now. I held and propounded that hope myself, thinking that fewer of us had managed to hide away from the virus until now than is the case. Mea culpa.
The particulars of my presentation were much like comments I made to open the Lifestyle Medicine 2020 conference (held virtually), and all about the “acute case for chronic health.” That message is, indeed, important– and remains fundamentally neglected.
Let’s be clear: SARS-CoV-2 is not, never was, and will not be a one-size-fits-all threat. Some of what increases risk, notably chronological age, is not modifiable. But much of what increases risk, especially for those who are biologically elderly but not chronologically so, is fundamentally modifiable. Many factors contribute to the tragic toll of COVID in the United States, but the poor state of our collective cardiometabolic health coming into the pandemic looms large among them.
That said, it is not the topic of my presentation that inspires this column, but rather the venue. I will avoid details for the sake of all concerned, but let’s just note that the “terms” agreed to in advance allowed for social distancing and mask use. The reality proved to be a packed conference room, no distancing whatsoever- and I the only one in the entire assembly with a mask. (Well, actually one fellow speaker, a colleague from California, had one as well- but he seemed inclined to meet the gathering half way, and wore it as a chin strap.)
Was this group oblivious, or ignorant? Not at all. They were well informed, wellness enthusiasts, and generally highly educated- including some number of PhD scientists, and attorneys in the mix. Nor was there anything very unique about this gathering in Ohio. I heard from a correspondent in Washington State about much the same inclination there; and from a colleague now in Oklahoma; and from a member of the Hasidic Jewish community in New York.
What’s going on?
Partly, these are the dire consequences of life in the post-truth era these past four years have fomented. When lies and truth compete for attention on a playing field that does no screening at the gate, truth often loses and trust always does. Public health runs on the concept of common interests and public good, and these in turn require trust in shared means to desired ends. Absent trust, the house divides into ruin.
But there is, I believe, more. I got an earful in Ohio about the blunt instrument of government action, the heavy hand of indiscriminate policy, and the general opacity in policy making that denies the public access to the data on which their elected officials were basing their decisions. Apparently innumerable communities all around the country harbor these same sentiments and impressions.
We could debate the legitimacy of such sentiments, but to what end? Ethics tells us my right to swing a stick ends where your nose begins. But the friction I saw was not about any one nose out of joint or stick out of place. It was an entire community of noses in agreement about the threat of swinging sticks from without. People feel as they do, and if we are to fare any better through what lies ahead, we must find some way to do so, together.
The problem here is as elaborate as the case made by Cass Sunstein in “Going to Extremes,” or as pithy as Newton’s third law: for every action, an equal and opposite reaction. If we view “lock it down” as the favored public health action to address the pandemic, “liberate it all” is the opposing reaction, and perhaps as inevitable as inertia. Certainly, so, in a world without trust to manage the native momentum of human impulse.
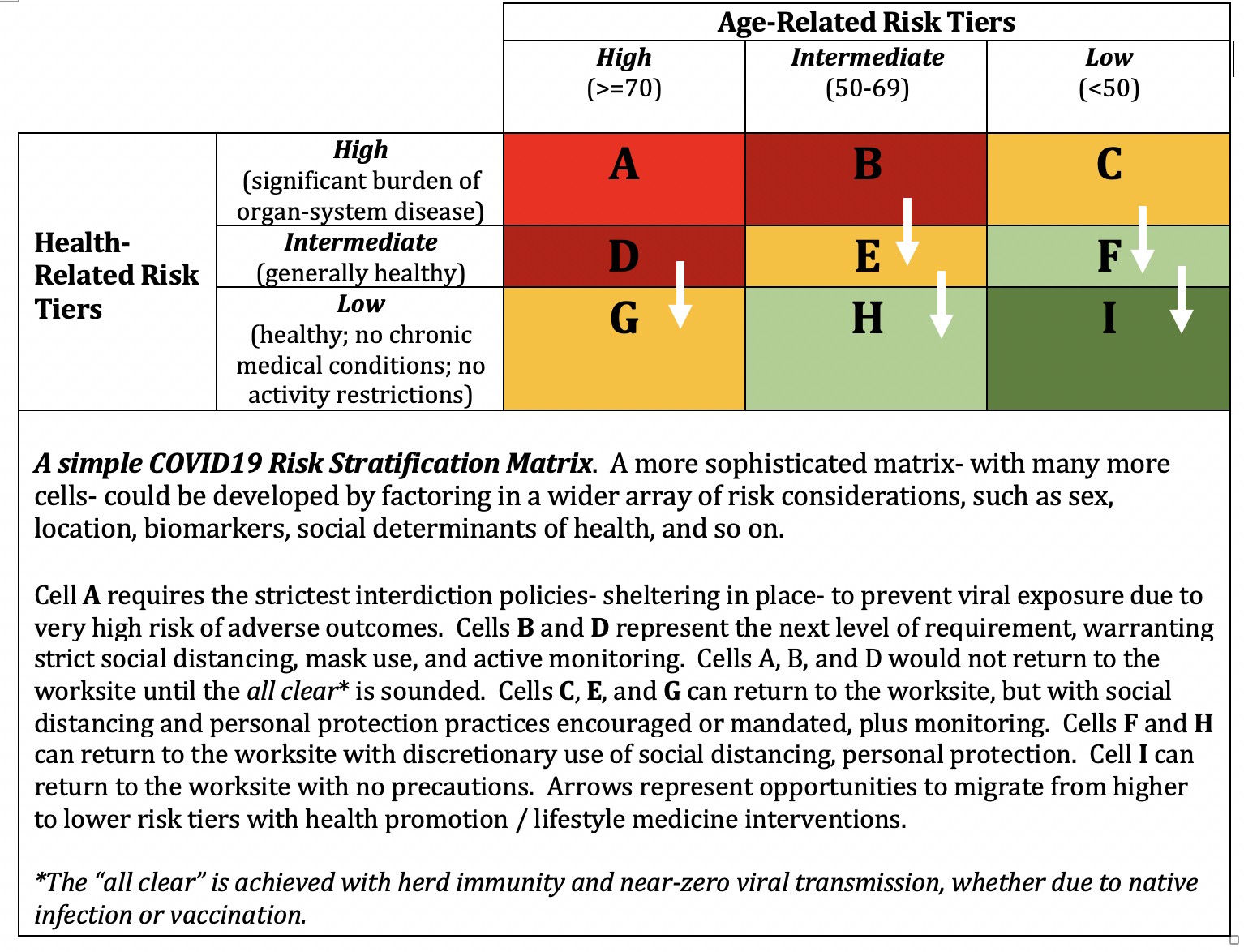
Which recalls to me the position I took those seeming lifetimes ago when the pandemic was new: total harm minimization, based on risk-stratified policies. Let everyone know you hear them; let everyone know you care. Let everyone know that any way the pandemic hurts them is bad, any way we can avoid such harm is good.
Our failure to inform our public health responses with temperate reasoning is by no means unique to COVID. Consider, for instance, the tumultuous national debate about the legalization of medical marijuana. How many with strong opinions in that melee knew that medical cocaine, fundamentally more dangerous, was legal all along? (In case you care to know, we use it in emergency departments to treat epistaxis- severe nosebleeds. Every ER I have ever worked in had a 7% solution of cocaine on hand in the pharmacy for that application- and it does the job well.)
Maybe legalizing an illicit drug for medical use sounds radical. But it is irrational not to ask: why was this drug, as opposed to some other, illegal in the first place? Are we being consistent about first principles, basing decisions on some consistent application of risk/benefit analysis?
Maybe total harm minimization sounds radical when dealing with a virus that can kill. But here, too, our inconsistency is glaring. Heart disease kills over 650,000 people a year in the U.S., nearly all of them prematurely- and dramatically so in many cases, cutting life short by years or even decades. These deaths are the unnecessary consequence of a culture that often favors corporate profit over public health. These deaths are….preventable. Why, then, no unified outrage in response to THESE deaths? Is it simply that, even for our most august public health champions, familiarity breeds contempt?
Perhaps you will note that we can transmit SARS-CoV-2 to an innocent bystander, but we cannot transmit heart disease, or diabetes. I beg to differ.
The distinction is just the medium of transmission. SARS-CoV-2 rides in water droplets and vapor. Heart disease and diabetes ride the memes and marketing collateral of a culture that runs on donuts, considers bacon a condiment, churns out new varieties of junk food to exploit the vagaries of fad and fashion, and peddles multicolored marshmallows to children for breakfast. Studies tell us of the propagation of obesity and chronic disease in social networks, presumably via memes, social norms, and the native human inclination to fit in. The so-called “chronic diseases” are, genuinely, transmissible- they just infect behaviors rather than lungs, assault ideas rather than immunity.
And they kill. They kill with indemnity. They kill at a scale far greater even than the worst case projections for the pandemic- and they do it year in, and year out. It will not end. There is no vaccine. They fill up hospital beds, and strain the ranks of health professionals. They encounter our complacency, and arguably even our contempt.
Perhaps the calls to protect every last one of us from COVID would garner more consistent support if the implied sanctity of life were not quite so condition specific, did not seem so arbitrary? Your death by COVID is a national calamity; your death by heart disease, stroke, diabetes…just another day of good business as usual in America.
I have long recited the parable of the Blind Men and the Elephant, courtesy of verse by John Godfrey Saxe, at the start of my talks. Saxe speaks of theology, but epidemiology is seemingly prone to the same: conflating the part for the whole.
I have long felt, but never more acutely than during the pandemic, like the seventh man- tagging along behind, with vision intact. A seventh capable of seeing what is right, and wrong, about the competing impressions of isolated parts of a greater whole. Seeing that everyone washing their baby, winds up with some dirty bathwater.
That central patch, taking in the full view, informs my unchanged position: we need to look both ways before crossing a busy pandemic, at the harms of infection, and the harms of our responses to it. We need to minimize both. While we are at it, we might be a bit more consistent about prioritizing human life if we expect people to believe us when we tell them that suddenly, every last one matters.
What a lonely place that centrist patch has proven.
I am not complaining; my plight is far better either than those laid low by this virus, or those with lives and livelihoods devastated by the social upheaval it has invited. But, lonely just the same.

Perhaps, at this late juncture, a vaccine will save us from ourselves. Perhaps the pandemic will burn itself out before ever we come together.
Any end to the pandemic will be better than none. But if we never find a way to see a common view of it, the tragic loss of life will be much compounded by the ravages of discord and distrust among the living. The injury of our losses will be demeaned in the insults we direct at one another.
My hope for it dims by the day, but there is a bigger view and a better way than this, or that. So says the seventh man.
-fin
This article was first published on LinkedIn.
Dr. David L. Katz is a board-certified specialist in Preventive Medicine/Public Health.
Click here to access the one-page summary of #TotalHarmMinimization
Click here to access the total harm minimization resource library
Click here to access a library of Dr. Katz’ “reality check” videos on the pandemic