
 Phases")
Alas, I think the current administration, despite appropriate respect for science and good intentions, is also bungling the pandemic, albeit in the opposite direction- perhaps an inevitable victim of inertia and Newton’s Third Law of motion. Yes, Omicron is spreading rampantly, and yes, hospitals are at capacity in many parts of the country. But it is clear the spread of Omicron cannot be contained; that both vaccination and the now highly prevalent state of prior infection by earlier strains of SARS-CoV-2 confer considerable protection against severe outcomes; that hospitalization is concentrated among the non-immunized and in particular among those with serious, prior, chronic conditions that place them at high risk of hospitalization this time of year, every year.
In such context, a continued emphasis on masking (certainly useful and valid in earlier pandemic phases when it made the short list of “all we had”) seems little more than window dressing now, cultivating the view that our government is making rules for the sake of rule making, no matter the futility- and imposing arbitrary restrictions and inconvenience. (Is there even a hint that masking has done anything to curtail the spread of Omicron or alter outcomes among the vast majority of us who have been vaccinated, with or without prior infection? I have found none.) If we are aiming to manage hospital quotas and save lives now, continued encouragement of vaccine uptake by the holdouts makes sense, but most effective would certainly be a whole new suite of care elements for the large populations of elderly, frail, and those with cardiometabolic and/or chronic respiratory diseases. Those care elements would include remote patient monitoring; telemedicine; active rather than passive surveillance for early indications of COVID infection; anticipatory distribution of approved COVID treatments for early and presumptive use among the vulnerable; and the concentration of confirmatory COVID testing in this population as well. Much of the testing now being done among asymptomatic populations is depleting resources that could be far better deployed; propagating confusion, consternation, and conflict; and clearly doing little to nothing to prevent transmission of Omicron, for many reasons that need not be enumerated here.
So, good intentions duly noted- but we, the people, are at this point at least as tired of futile pandemic doctrine as we are sick with Omicron.
Here we are– two full years into this public health stress test we have failed in every way imaginable- and it’s best we understand why. We are living through the calamitous follies of history, and unless we learn from them, we are prone to repeat them. Once has been more than enough, thank you.
The common, rhetorical roots of “response” and “responsibility” are, I trust, self-evident. Less evident perhaps is that neglect of that immanent link- born of etymology, but nurtured in application- is tangled in the roots of our grand pandemic failures.
That we have failed to manage this pandemic is also, I trust, self-evident. Despite the bounties of drama, activity, anxiety, and opinion- we have largely failed to save vulnerable lives or livelihoods. Before the advent of vaccines, the most vulnerable were inadequately protected, and died in droves- as they are again filling hospitals now. Whatever deaths we prevented in any pandemic moment, we mostly just deferred to the next when our reactions were ill-timed, inadequate, excessive, or misdirected. We sheltered and emerged with want of clearly articulated guidance, goals, or timelines; and want of the essential choreography, dictated not by whim, but by such critical considerations as incubation period. We were all enlisted in pandemic theater, with little genuine gain to show for it.
We did little to establish policy goals directed at minimizing pandemic harms not resulting directly from infection- such as the explosive increase in addiction and its consequences. And we did nothing to address the underlying, and modifiable, poor cardiometabolic health putting a majority of Americans at higher risk of dire COVID outcomes than need be. That sad and costly deficiency persists to this day, and bears repeating: we had a prior pandemic of cardiometabolic disease that made COVID vastly worse than it needed to be, and have ignored that fact and its implications as if lives depended on it. They did, and those lives- we have mostly lost.
But by far the biggest failure is what we cannot blame at all on the vagaries of viral transmission. That is the failure to come together in common cause, and there- the fault lies not with SARS, but entirely with ourselves.
We find ourselves, these 2 years into this shared experience of a historic public health crisis, a house divided by riven visions, discords, and distrust. We are at the very edge of open rebellion, civil unrest, and perhaps even- shocking as it is to say- civil war. Other currents were roiling in these directions before COVID, of course, but COVID-related dysfunctions have brought them to flood.
I contend that the neglected connections among risks, policy responses, and the even-handed assignment of responsibility are the incubator of this blight. For, had we honored the links between pandemic response and responsibility, and cultivated respect where we have instead sown rancor- we could, and I believe, would derive the unity required to meet this, and other challenges, too. Maybe that’s just hope talking; but hope always deserves an ear. Or perhaps I’ve just seen too many of those fantasy movies, where we come together against some great and common threat, and prevail.
There were, arguably, four basic pandemic phases, summarized below. Each has distinct implications for the imperatives of response, and the assignment of responsibility. We heard, of course, nothing remotely like this about the requisite laps in this relay race- predictably, not from the prior administration; and more sadly, not from the current one either.
Phase 1: risks largely unknown; responses unestablished
o Imperatives: establish and declare primary policy objective(s); generate estimates of risk and corresponding remedial actions
o Responsibility: with federal authorities
o Timeline: the first several weeks of pandemic response
Phase 2: general risks estimated; general responses recommended
o Imperatives: use real-time data capture to quantify risks to the population, and articulate “best practice” defenses
o Responsibility: with federal authorities for guidance, and mandates directed to most vulnerable; some sharing with general population for uptake and application
o Timeline: the first several months of pandemic response
Phase 3: stratified risks established, specific responses recommended and supported
o Imperatives: enable every individual to know personal risk of adverse COVID outcomes, best means of reducing risk and practicing self-defense; ensuring resource availability
o Responsibility: resides with government officials and private sector experts to generate personalized guidance and ensure resource access, but resides mostly with individuals for uptake and application. Exceptions- mandates- still warranted for highly vulnerable populations.
o Timeline: after the first several months of pandemic response, until the widespread availability of definitive protections (e.g., vaccines)
Phase 4: refined, stratified risks established; specific defenses deployed, refined recommendations issued
o Imperatives: refine means of personalized risk assessment, make available definitive defenses (i.e., vaccines)
o Responsibility: as for Phase 3 initially, but once time provides opportunity for everyone so inclined to take advantage of vaccination (and, subsequently, boosters), the argument of being vaccinated to protect others no longer pertains, since everyone has the option to protect themselves. Individual responsibility prevails here, with authorities focused still on resource deployment to the most vulnerable populations (e.g., ensuring effective drugs for early COVID treatment are available at all nursing homes) and on ensuring health system surge capacity.
o Timeline: upon the advent of definitive protections (i.e., vaccines)
Phase 1 was in late 2019 and early 2020, when we learned of SARS-CoV-2, first in Wuhan, then in Seoul, and then in Lombardy, Italy. At the first indications of a significant threat, a Camp David Summit should have been convened by the federal government, calling on a who’s who in public health, clinical medicine, epidemiology, virology, chronic disease management, hospital administration, supply chain management, social determinants of health- at a minimum. The imperatives of this Summit, reasonably held concurrently with a vigorous attempt at a brief, but serious, national lockdown should have been: protect the population while establishing the single overriding objective of pandemic response; establish risk estimates; and generate initial guidance.
The single overriding objective should have been: total harm minimization. What else? I welcome rebuttals, but it’s hard to imagine any viable alternatives. All that followed, should have followed in service to that objective.
Phase 1 responsibility resides all but entirely with the federal authorities. I think even the most ardent libertarians would concede that, and even respect it- if the government at the start made clear that Phase 1 would be organized, disciplined, and as brief as possible- before yielding to phase 2.
Phase 2 would ensue when the Summit was done, risks estimated, and suitable responses enumerated. As an example, the evidence from Italy, Korea, and China already indicated in very early 2020 that frail elderly were at extreme risk of bad COVID outcomes- while the disease was generally mild in young, healthy people. Among those early responses should have been meticulous protection of highly vulnerable populations- especially in nursing homes. As obvious as this seems, it (a) did not happen, and (b) has been stunningly excoriated in caricature. This very idea- letting remedy match risk, as punishment is famously encouraged to fit crime- was what I called “vertical” or risk stratified interdiction and what the Great Barrington Declaration (wrongly notorious, in my view) called “focused protection.” Neither, despite the diatribe, espoused a “let it rip” approach to the pandemic. Both articulated the need to match response to risk. Period. Of note, that is how medicine and public health always operate, or did- until now.
In Phase 2, the government would still own a fair share of responsibility for standardizing responses, disseminating guidance, ensuring relevant supplies (e.g., masks and other elements of personal protection), establishing protocols, and as rarely needed- enforcing these. But armed with information about risks and reasonable defenses, even in this early phase individuals could have been called upon to gauge their personal risk and choose their protections from a menu of options. I believe even small indications of respect for autonomy would have gone a long way.
Perhaps you think we could not count on people to “behave well,” because so many people have not behaved well. But I believe using this to rationalize the one-size-fits-all, heavy handed futilities of our pandemic management is putting the cart before the horse. The horse here was an early failure to establish and socialize a decisive goal, delineate responsibilities, honor the diverse forms pandemic menace could take, or project what phases of response would follow. Amidst such opacity, who can blame those who boarded the cart of distrust? We reaped distrust, because we sowed distrust.
In Phase 3, several months into our pandemic experience at most, we could rightly expect- had the federal authorities and private partners done their jobs- stratified risk estimates, specific “best practices” defined by risk tier (and based on careful scrutiny of the full, global experience), and a host of resources to empower our personal protections- from daily updates on a dedicated Department of Health web page, to sourcing of relevant materials.
And, of course, this was the time for a nationally coordinated “let’s get healthy, America” campaign, to address that neglected, massive burden of chronic disease, cardiometabolic risk factors, and obesity making all of this so much worse than it needed to be.
The idea of risk-stratifying the COVID pandemic is far from daunting. I created a crude, but basically robust, color-coded risk matrix in the very early going (shown below- including elements in the legend that are now clearly out of date). Associates developed a far more sophisticated on-line risk calculator to quantify personal risk, and show best how to attenuate it. The authorities did neither.
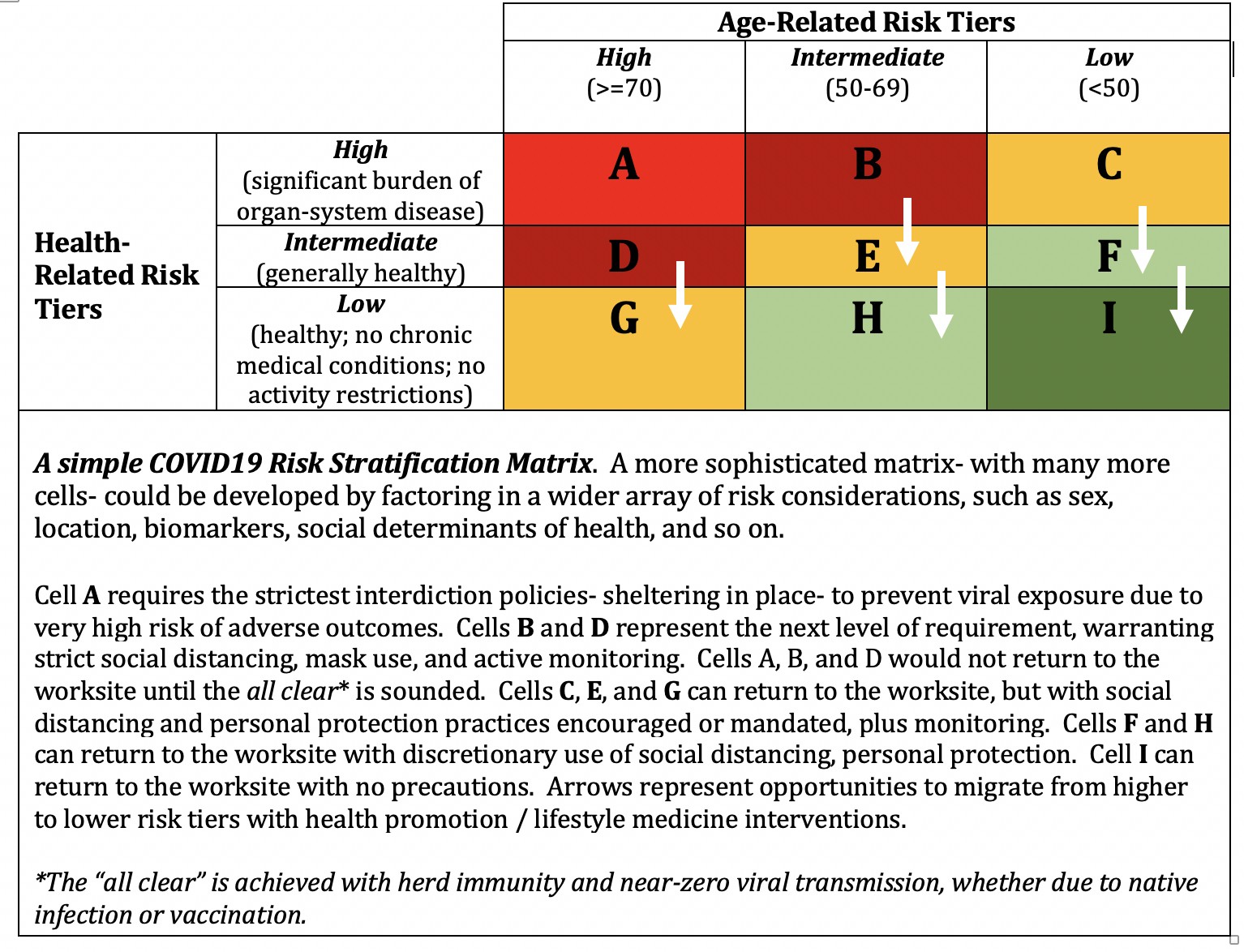
Imagine if a universally accessible and widely promoted government site had been established to help each of us know our risks and risk factors; to guide us on tailored, personalized defenses matched to risk; and – importantly- to help us address and modify those risk factors, too, whenever plausible. Advanced age cannot be modified, but all of the other risk factors for bad COVID outcomes- obesity, hypertension, diabetes, heart disease, and so on- can be. Why on earth was this systematically neglected and ignored?
By Phase 3, the government should have embraced responsibility for helping everyone so inclined to know, and lower, their COVID risk. And along with that – they should have turned over much of the responsibility for acting on those opportunities to individuals. This is how everything in public health works.
Poor diet quality kills over 500,000 of us prematurely every year (it is, in fact, the single leading risk factor for premature death in America today, and throughout the modern world)- and contributed mightily to the toll of COVID, both indirectly via the chronic diseases it feeds, and directly as well. Yet, we hear no talk of a national take-over of our dubious, and willfully manipulated, food supply. What we get instead is guidance from authorities, and reliance on action by individuals. From my perspective, we have too little policy constraining the harms of profitable junk masquerading as food. And obviously, food is not an infectious agent (although diet-related chronic diseases are, in fact, transmissible via social networks). But some consistency in how we handle the assignment of responsibility with lives on the line is certainly in order. The principle of autonomy makes a bad trifle.
Phase 4 would follow with the advent of vaccines. With the availability of genuinely safe and effective vaccines, the government’s primary responsibility shifts to defining eligibility, and making them available to all candidates as efficiently as possible. But with this “high level” defense now deployed, the government might have conceded responsibility for managing the lesser defenses such as masking, to individuals.
By way of analogy, authorities might be responsible for ensuring a strong, protective barrier at the edge of a great precipice on public land – a viewing station overlooking the Grand Canyon, for instance. Before the barrier, there might have been alternative requirements, or at least recommendations, to reduce the risk of calamitous fall. After the barrier, however, I don’t think the park authority need mandate our choice of shoes. Perhaps a shoe requirement makes sense before the protective barrier is erected (e.g., no flip-flops allowed!), but after- it is an inconsequential addendum, and a decision rightly deferred to individuals.
Pandemics are global. All of these ruminations on national responses and the assignment of responsibility should actually be global, mediated via the WHO and UN. My hope, however, could not triumph sufficiently over experience to feed that lofty aspiration even a crumb. National cogency is the fallback position. Global unity, however much a truly effective pandemic response screams out for it, seems preposterously out of reach for us fractious humans, alas.
Divisive antipathy is unhelpful in managing a pandemic, to put it mildly. But this is not one calamity, it is several- of which the pandemic is the least.
This civil rift incubates a host of dangers. Long after this pandemic ends, it will matter beyond measure whether the United States of America is a representative democracy, or something sinister and different. That threat plays out in plain sight now, and our divisions are aiding and abetting. There is misguided fretting and absurd conspiracy theories about the shadowed autocratic inclinations of those advocating social restrictions and vaccinations in response to the pandemic, while a full, frontal assault on democracy with just such intentions marches through daylight. Lockdowns, however intrusive, inelegant, and ineffective, have genuinely been about protecting us. There are no mind-controlling microchips in vaccines. An open assault on the seat of government makes its way through the fog of pandemic nonsense.
And even that, colossal though it is (who among us could even imagine a day when democracy, fair elections, and peaceful transfer of power in the United States of America could be in jeopardy?)- is not the greatest toll of our divisions. The greatest toll by far is the genuinely existential threat of what we keep doing to the planet and climate, perpetuating abuses to a refrain of “blah, blah, blah.” This one, and only this one, invites us to look up “ELE.”
Such are the grim progeny of distrust and disunion. We watch fantasy movies to see how a common threat brings us all together. We are living a common threat, and life is diametrically opposed to the wishful thinking of such art.
Had we reached “now” with clearly articulated objectives- notably, a commitment to total harm minimization; a phased and transparent approach to responses and responsibilities; and an explicit commitment to translate as much responsibility as possible from federal authorities to individuals as soon as possible- I think we could have reached here together.
Launching into pandemic response policies with no articulated objective- never made sense. Just “flatten the curve” with no projection of plans to follow- never made sense. Mask and other mandates to protect one another made perfect sense when greater means of self-defense were not available. Now that everyone who chooses to be vaccinated and boosted can be, these policies are, at best, questionable- and questioning them should not be deemed subversive.
So much effort directed at the consequences of infection, with infection now all but inevitable as Omicron circulates widely, with none directed at the underlying causes- chronic cardiometabolic diseases and obesity- makes no sense.
Revising policy on the fly, always a step behind the relentless spread of Omicron, makes no sense- as it propagates confusion, consternation, and even more distrust. Perhaps, even, disgust.
Guidance, guidelines, requirements, and mandates of a “one-size-fits-all” variety have not made sense since the advent of Phase 2, but make far less sense now that tens of millions of us have had COVID, many of us more than once, and derived natural immunity. For us, our first vaccine was a booster; our second vaccine, another booster. Where is the informed federal guidance that acknowledges this fundamental distinction? Its omission feeds into daft conspiracy theories about government overreach, and profiteering by Big Pharma (the latter is likely true, but does not belie the value of vaccines). I think it is clumsy ineptitude rather than maleficence, but it’s a bad look just the same. In short, it makes no sense.
If we want everyone to follow the same science, it would help a lot to make a bit more sense applying it.
Yes, hospitals are now filled to bursting. But partly this is a seasonal trend, partly it is the result of vaccine resistance only made worse by the distrust we’ve fomented, and largely it is due to the neglected, prior burden of chronic disease. Reports indicate many people in our hospitals now “with” COVID are not in “for” COVID. They test positive, incidentally, for Omicron, but are hospitalized because of the usual scourges: diseases of heart, lung, and metabolism- compounded by otherwise mild viral infection.
We might have arrived here together.
Instead, we stand now at the brink of that precipice, eyeing one another with suspicious contempt, pushing one another, jostling for position, and in some quarters- vandalizing the protective barrier. Such is the spawn of opacity where transparency might have been; of missed opportunities to show respect; of failure to honor the various claimants to responsible action.
Instead of enjoying a common view of America the Beautiful to a rousing chorus of Kumbaya- we are in great disarray and grave danger. The barrier is in ruin, and many in the restive, jostling crowd are wearing just the wrong kind of shoes- because exasperation is an enemy to reason. The risk grows by the minute of toppling into the void.
Here’s to the triumph of hope over this experience.
-fin
This article was first published on LinkedIn.
Dr. David L. Katz is a board-certified specialist in Preventive Medicine/Public Health and at this point, a certified COVID curmudgeon.
Click here to access the one-page summary of #TotalHarmMinimization
Click here to access the total harm minimization resource library
Click here to access a library of Dr. Katz’ “reality check” videos on the pandemic