

We do, now, have the lesser opportunity to clean up the crash site, and put viable train cars back on salvaged tracks. With a new administration poised to sound the “all aboard,” what place of promise should be our shared destination?
With over 100,000 new cases nationwide reported daily over a string of recent days, we must concede that containing viral spread at the level of the general population is no longer possible. That chance came and went with the one-two punch of too-late lockdown at the start of all this, too-random and indiscriminate reopening several months later. Almost everyone can now be a source of SARS-CoV-2, and absent each of us in the entire population suffering a veritable solitary confinement for longer than the incubation period of this virus, its purchase on the population is insurmountable.
But as I have argued from the start, cases are not the real concern; casualties are the concern. Infection that causes no harm to the person infected or anyone else is inconsequential. Infection that causes any genuine harm – severe symptoms, hospitalization, lasting complications, death, or any of those as the result of transmission to someone more vulnerable – is our common enemy and the rightful target of our every interdiction effort.
The current prevalence of infection in the United States may not be as great as it seems, and is almost certainly not as much greater now than at the start of all this, as current data imply. The former is true because the commonly deployed PCR test is sensitive enough to detect residual viral fragments and potentially misrepresent them at times as active infection when that is no longer the case. When both prior and current infections are lumped into one diagnostic category, there is every reason to expect a big bump in prevalence.
The latter is true because while we are still testing too little, we are testing massively more than in the early going, when mild and asymptomatic cases of SARS-CoV-2 were sure to be overlooked entirely.
Even making allowance for all that, however, the prevalence of infection makes complete population-level containment implausible at this time. Here is what we can, and in my view should, do now.
1) Risk stratify the population with regard to adverse outcomes of SARS-CoV-2 infection. Every American should know their personal COVID “risk tier” and that of their loved ones. This could be as coarse as “high, medium, low;” or as granular as a numerical scale, even a percent probability of hospitalization or death if infected.
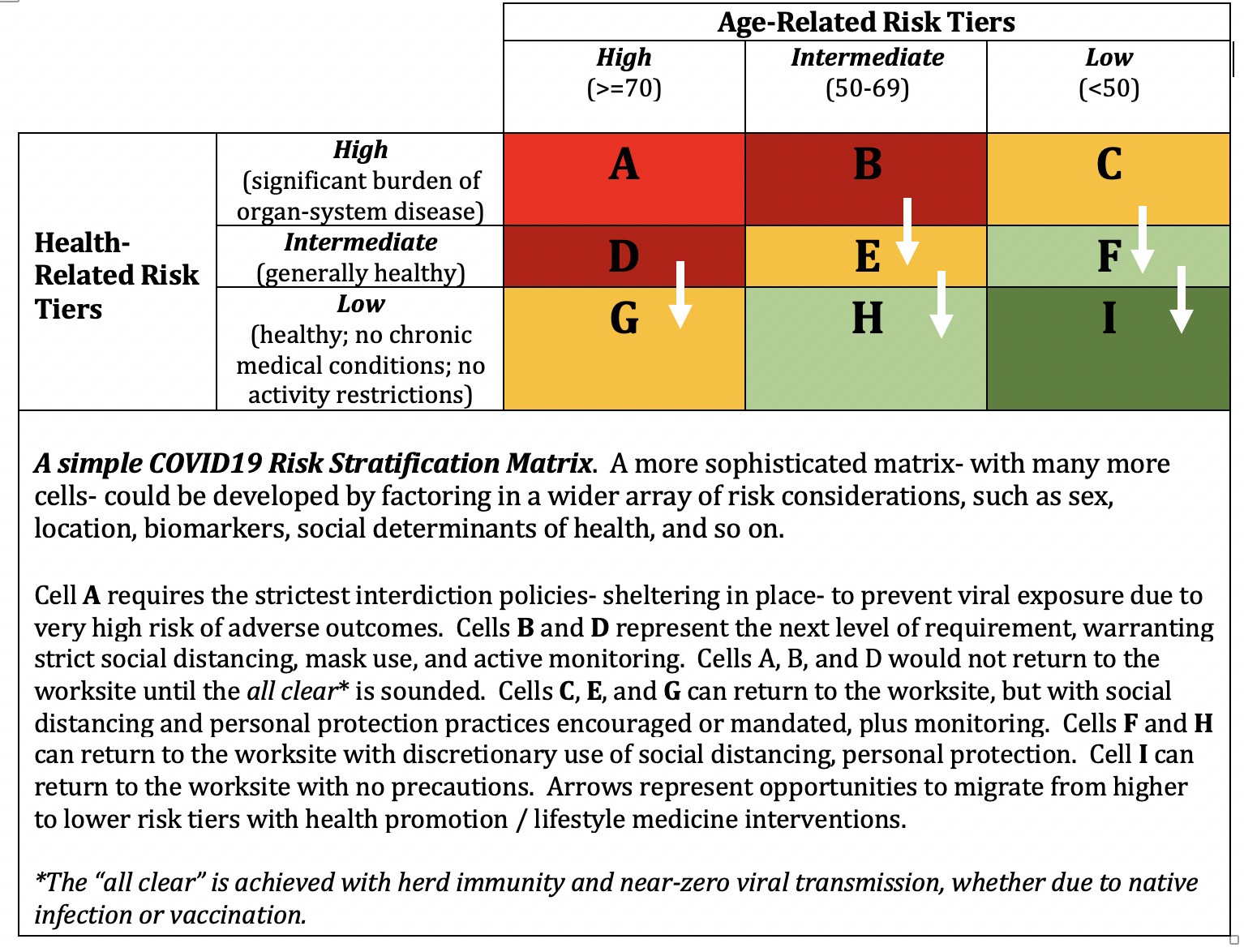
2) Issue specific guidance for policy and practice directed to risk status. This guidance should pertain not only among households, but within households where risk tiers mingle. Simplistically, policy and practice in every situation should accommodate the requirements of the highest-risk individual in the mix. A fully developed expression of this should be a simple, user-friendly, interactive web site where a family can characterize their composition – and get a “personalized” set of recommendations/guidelines to minimize the risk of any COVID harms.
3) Finally, the single most neglected element in the national response to COVID is the acute case for chronic health. SARS-CoV-2 devastatingly exploits America’s massive burden of preventable, and reversible, chronic disease. The amelioration of cardiometabolic health in this country always offered the “chronic” benefit of adding years to life, and life to years. It now superimposes the acute benefit of reduced COVID risks, potentially by many multiples. The opportunity to attenuate the pandemic toll by means of a national health promotion effort cannot be overstated, yet with rare exception has barely been stated at all. Now is not a moment too soon to fix that.
That, then, is what the immediate refurbishment of our national COVID crash site entails. Clean up, reconstruction, and the resumption of forward progress are represented by comprehensive risk stratification; personalized guidance corresponding to risk; and the substantial attenuation of risk by means long known to us.
In the interim, of course, we should all embrace the obvious sense and accruing science that both support distancing and mask use. These practices of basic decency and mutual respect do not obviate viral transmission entirely, but at a minimum attenuate exposure dose– and that matters. The elderly and those with significant chronic illness should be doing all they can to avoid potential exposure, while awaiting further guidance. Advances in treatment, and an eventual vaccine, remain key components of the overall response.
We cannot undo the early crash, but we can avoid the burn. We have the wherewithal to re-lay tracks and re-right cars. And then, for what lies between us and the inevitable end of this pandemic, a venerated bit of Americana is perfectly apt: Let’s Roll.
-fin
This article was first published on LinkedIn.
Dr. David L. Katz is a board-certified specialist in Preventive Medicine/Public Health.
Click here to access the one-page summary of #TotalHarmMinimization
Click here to access the total harm minimization resource library
Click here to access a library of Dr. Katz’ “reality check” videos on the pandemic